Some thoughts on clinical IT systems & Electronic Medical Records
22/01/13 07:15
Recently a team from West Suffolk NHS Foundation NHS Trust spent (a tiring) 48 hours in Boston and Connecticut to look at a potential IT system. Our team included our finance director, IT director, an orthopaedic surgeon and myself as medical director and consultant surgeon.
We visited MediTech and one of its customers, the William Backus Hospital in Norwich, Connecticut.
Like most UK hospitals we have an ageing PAS system that isn’t fit for modern medicine, alongside which we run a disparate range of isolated clinical & administrative IT systems, all with varying logins etc. Many of these systems work very well but they don’t work seamlessly and they certainly aren’t integrated. Our PAS system has to be replaced and the key issue will whether we simply replace our PAS and keep our existing clinical systems or whether we implement an integrated system. And then there’s the small matter of how we pay for it all…
I’d like to thank all the staff of William H Backus Hospital and of Meditech for all their help, advice and professionalism.
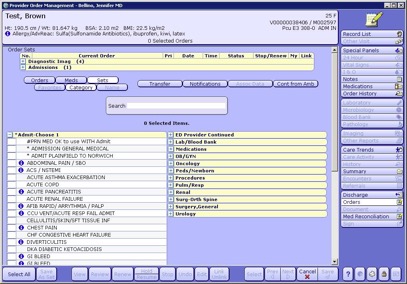



We visited MediTech and one of its customers, the William Backus Hospital in Norwich, Connecticut.
Like most UK hospitals we have an ageing PAS system that isn’t fit for modern medicine, alongside which we run a disparate range of isolated clinical & administrative IT systems, all with varying logins etc. Many of these systems work very well but they don’t work seamlessly and they certainly aren’t integrated. Our PAS system has to be replaced and the key issue will whether we simply replace our PAS and keep our existing clinical systems or whether we implement an integrated system. And then there’s the small matter of how we pay for it all…
So what did we learn?
In no particular order:- A single integrated system that does everything has huge potential quality benefits
- One password!
- Making a purely financial business case (even allowing for productivity gains) is going to be tough
- The quality benefits can help the business case but the money spent won’t be available to spend elsewhere
- Using IT systems to avoid variation between clinicians
- Implementation of any such system is a major undertaking and would primarily be a clinical change project not an IT project
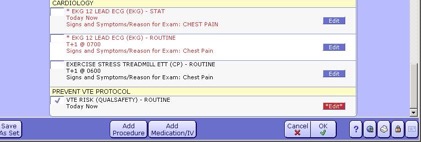
- Majority of effort in drafting “care orders” or protocols tied to chief complaint
- Ask clinicians "what do you want to see?"
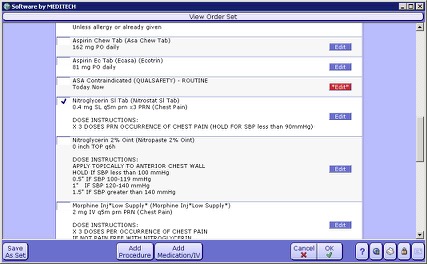
- ALL the relevant clerking fields, investigations, instructions to nurses, prescriptions are prompted all ordered with single click
- Maintains standard levels of care
- Develop standard templates to match specialty needs
- Can monitor clicks needed to achieve critical tasks, with view to minimising them
- These systems are expensive and so will the time of clinicians that is necessary to get the most out of them
- Doctors initially resistant e.g. “"why do we have to do this?" but done properly they start saying "Why aren't we doing x,y or z?"!
- Now doctors leading change and it’s attractive to best young doctors
- Patients are becoming ever bigger users of their own data. They want to take an active role in health care and you need a patient/consumer portal
- There’s a LOT more money available to spend on IT and hardware in US hospitals
- Contrary to my personal experience, voice recognition can work. I’m going to have to give it another try!
- For e-prescribing need to avoid "alert fatigue"
- The ONLY mandatory field to request a test is the reason for the test
- Ward rounds start off slower but get faster than writing (but takes a YEAR!)
- When you get the IT right then it's easier than paper, if it’s not right then problems multiply
- Dedicated physician support phone available 24 hours
- IT rep available on the floor for first few days (after training)
- Can tailor results notifications, e.g. nephrologist could ask to be told only about specified change in blood results rather than every high urea & low Hb
- Hospitals have new post of Chief Medical Information Officer responsible for clinical content who is first port of call for doctors to raise issues
- Single patient history in hospital and in community
- It’s incredibly frustrating that that it’s so hard for hospital & GP systems to communicate with each other
- There must be national standards for data transmission
- Same screen wherever you go in organisation
- Can't run a hospital without an integrated system to generate automatic regulatory reports
- IT manager knows its working because of lack of complaints (from doctors!)
In conclusion
I think that clinicians would love a single integrated clinical IT system and there are a lot of significant quality advantages. We need to crack the problem of communication between different systems in primary & secondary care. Implementing such a system would be a huge clinical change project. And I still don’t know if we can afford it, but I now wonder if we can afford not to.I’d like to thank all the staff of William H Backus Hospital and of Meditech for all their help, advice and professionalism.
blog comments powered by Disqus